Expert Opinion BCV
It cannot always be clearly distinguished whether it is the BCV or in fact the SCV which is being punctured via this access (2). However, clinically it does not matter as the puncture of any of these veins at this site provides a rather direct line to the superior caval vein. Both veins are fixed to the clavipectoral fascia avoiding anterior vessel wall collapse under the pressure of the approaching needle. It seems to be easier to cannulate the left BCV. This could be related to the different anatomy (3). The right BCV is in most cases much shorter than the left one. The right BCV also quickly takes a sharp angled, caudad turn whereas the left one runs first in a significantly less caudally directed, more horizontal way (BCV-Figure 2, 3xxx).
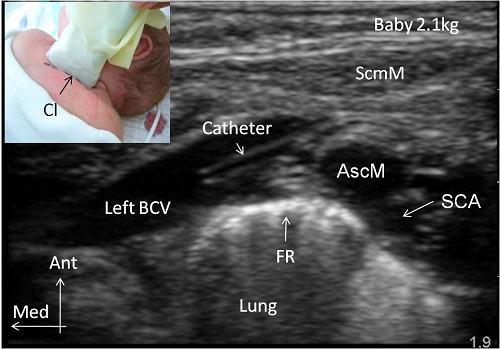
BCV-Figure 2
BCV-Figure 3
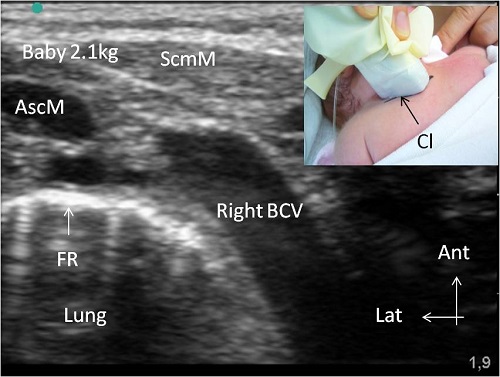
Both the usually shorter distance as well as the sharp angled, caudally orientated right BCV could explain its more difficult ultrasonographic imaging in the longitudinal axis (BCV-Figure 2,3xxx) . Delineating the longitudinal axis of these veins via US requires a slightly more caudally orientated US probe placement for the right BCV (BCV-Figure 2, 3xxx). This apparently makes a good view of the needle advancement in the in-plane technique more difficult for the right BCV above all in neonates. In addition the left BCV is apparently larger than the right one in preterm babies (4). The major advantage of the supraclavicular in-plane technique is the view of the advancing needle over more or less its entire distance and directing it under real time US control into the longitudinally imaged BCV without any disturbing US shadow caused by the clavicle (1, 2).
The major disadvantages of this method is that the in-plane technique requires that the needle be located inside a 1-mm longitudinal area (1). This necessitates excellent hand-eye coordination which may be even more difficult for the right BCV due to the slightly more caudally orientated US probe placement.