Ilioinguinal/iliohypogastric block
Dr Richard Craig
Content
- Introduction
Indications
Specific contraindications
Anatomy
Technique
Volume of LA
Specific complications
Bibliography
Indications
The ilioinguinal-iliohypogastric nerve block provides intraoperative and postoperative analgesia for inguinal surgery.
It may be useful for providing analgesia for:
- Inguinal hernia repair
- Orchidopexy
- Hydrocoele repair
- Varicocoele surgery
It has also been used, in combination with T11 and T12 intercostal nerve blocks, to provide post-operative pain relief after renal transplant. (1)
Its use in adult patients undergoing laparotomy via a Pfannenstiel incision did not result in a reduction in pain score, length of hospital stay, or postoperative morphine consumption. (2)
The block is also used in chronic pain management for patients with persistent inguinal post-herniorrhaphy pain, however, a recent study concluded that the block was not useful for either the diagnosis or management of this condition. (3)
Specific contraindications
Local infection
Anatomy
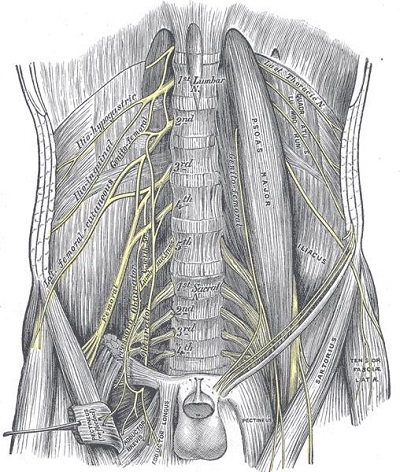
- The ilioinguinal and iliohypogastric nerves form part of the lumbar plexus.
- They are branches of the primary ventral ramus of L1 and receive a branch from the 12th spinal nerve.
- The L1 primary ventral ramus enters the upper part of psoas major where it branches into the ilioinguinal and iliohypogastric nerves.
- The nerves emerge at the lateral border of psoas major and pass anterior to quadratus lumborum. They pierce the lumbar fascia at the lateral border of quadratus lumborum and run in the plane between the internal oblique muscle and transversus abdominis muscles.
- The iliohypogastric nerve runs superior to the ilioinguinal nerve.
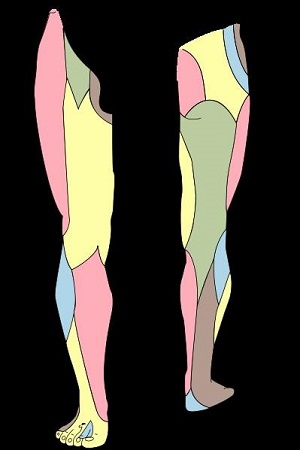
- The iliohypogastric nerve divides into a lateral cutaneous branch and a medial (or anterior) cutaneous branch at the level of the iliac crest. The lateral cutaneous branch pierces the internal and external oblique muscles immediately above the iliac crest to supply skin of the gluteal region. The medial cutaneous branch pierces the internal oblique muscle and external oblique aponeurosis to supply the skin above the inguinal ligament and the suprapubic region (i.e. the hypogastric region).
- The ilioinguinal nerve pierces the internal and external oblique muscle to reach the lower border of the spermatic cord or round ligament of the uterus and enters the inguinal canal. It supplies sensation to the skin of upper medial thigh and the upper part of the scrotum and root of the penis or the skin over labium majus and the mons pubis.
- A study of 25 neonatal cadavers measured the distance from the anterior superior iliac spine (ASIS) to the ilioinguinal and iliohypogastric nerves on a line connecting the ASIS to the umbilicus. (4) The left and right ilioinguinal nerves were 1.9 ± 0.9 mm (mean ± SD) and 2.0 ± 0.7 mm (mean ± SD) from the ASIS. The left and right iliohypogastric nerves were 3.3 ± 0.8 mm and 3.9 ± 1.0 mm from the ASIS.
- An ultrasound study involving 50 patients with a mean age of 40 months and a mean weight of 13 kg, reported a mean distance from the ASIS to the ilioinguinal nerve of 6.7 (SD2.9)mm, and a mean distance from the ilioinguinal nerve to the peritoneum of 3.3 (SD1.3) mm. (5)
- The fascial plane between the transversus abdominis muscle and the transversalis fascia is in continuity with the space around the femoral nerve.

Technique
Ultrasound-guided
Position the patient supine.
Use a high frequency linear probe (10Mhz or greater).
Place the probe on the anterior abdominal wall along the line joining the anterior superior iliac spine (ASIS) and the umbilicus.

Position the probe such that the bony shadow from the ASIS is visible on one side of the image on the screen. Identify the peritoneum, transversus abdominis muscle, and internal oblique muscle. The external oblique muscle may not be visible as a distinct muscle layer at this level.
Sliding the probe in a cephalad direction up over the iliac crest, whilst maintaining the orientation of the probe along a line to the umbilicus, will bring all three muscles into view as three distinct layers. This may be useful if there is any doubt about the anatomy and the relevant planes. Always identify the deepest structures first (i.e. the peritoneum) and work toward the superficial structures to identify each layer.
The ilioinguinal and iliohypogastric nerves are seen in close proximity to one another as two small round hypoechoic structures with a hyperechoic border. They lie in the plane between the internal oblique muscle and the transversus abdominis muscle close to the ASIS (in a study involving 50 children of mean age 40 months the mean distance from the ilioinguinal nerve to the ASIS was 6.7 mm). (5)

REMEMBER TO ALWAYS IDENTIFY THE MUSCLE LAYERS FROM THE INSIDE OUT.
Perform a dynamic scan, adjusting probe angle, the gain, and the depth to obtain the best possible image of the nerves and surrounding structures.
Note that it may not always be easy to visualise the nerves due to the variability of nerve anatomy distal to the midaxillary line, if in doubt place the local anaesthetic in the transversus abdominis plane.
Insert the block needle in plane from medial to lateral and ensure that there is a good image of the needle tip at all times as the needle is advanced. Deposit local anaesthetic around the nerves in the transversus abdominis plane.
Landmark technique
This block has a high failure rate and complications such as femoral nerve block and peritoneal puncture are more likely than with the ultrasound guided block (5). In a study of 50 children of mean age 40 months the mean distance from the ilioinguinal nerve to the peritoneum was 3.3 mm (5).
The needle insertion point should be approximately 2.5 mm (range 1.0 – 4.9mm) medial to the ASIS on a line drawn between the ASIS and the umbilicus (4). Use a short bevelled needle. Insert the needle just through the skin into the subcutaneous tissues and then advance the needle slowly until a fascial click or loss of resistance is felt. This occurs as the external aponeurosis is pierced. Inject the local anaesthetic at this depth, between the external and internal oblique.
Volume of LA
In expert hands as little as 0.075 ml/kg of 0.25% levobupivacaine for ultrasound guided blocks (6).
0.3 ml/kg of 0.25% levobupivacaine for the landmark technique (5).
Specific Complications
Block failure (up to 30% is some series using the landmark technique (5))
Colon puncture, small bowel puncture, pelvic retroperitoneal haematoma, bowel haematoma,
Transient femoral nerve palsy with transient quadriceps paresis. The latter complication has an incidence of up to 6% with the landmark technique (7). The quadriceps paresis resolves within hours.
Bibliography
1. Shoeibi G, Babakhani B, Mohammadi SS. The efficacy of ilioinguinal-iliohypogastric and intercostal nerve co-blockade for postoperative pain relief in kidney recipients. Anesthesia & Analgesia. 2009. Vol. 108, 1, pp. 330-3.
2. Wehbe SA, Ghulmiyyah LM, Dominique el-KH, Hosford SL, Ehleben CM, Saltzman SL, Sillis ES. Prospective randomized trial of iliohypogastric-ilioinguinal nerve block on post-operative morphine use after inpatient surgery of the female reproductive tract. Journal of Negative Results in Biomedicine. 2008. Vol. 7, 11, p. 1477.
3. Bischoff JM, Koscielniak-Nielsen ZJ, Kehlet H, Werner MU. Ultrasound-guided ilioinguinal/iliohypogastric nerve blocks for persistent inguinal postherniorrhaphy pain: a randomized, double-blind, placebo-controlled trail. Anesthesia & Analgesia. 2012. Vol. 114, 6, pp. 1323-9.
4. van Schoor AN, Boon JM, Bosenberg AT, Abrahams PH, Meiring JH. Anatomical considerations of the pediatric ilioinguinal/ iliohypogastric nerve block. Pediatric Anesthesia. 2005. Vol. 15, pp. 371-7.
5. Willschke H, Marhofer P, Bosenberg A, Johnston s, Wanzel O, Cox SG, Sitzwohl C, Kapral S. Ultrasonography for ilioinguinal/ iliohypogastric nerve blocks in children. British Journal of Anaesthesia. 2005. Vol. 95, 2, pp. 226-30.