Femoral Nerve Block
By Dr Jacinth Tan
- Fast, safe and effective procedure.
- In patients undergoing surgery: Reduces the amount of general anaesthetic and opioid analgesics needed intraoperatively1, reduces post-operative pain and analgesic consumption1, 2, and may even reduce the length of hospital stay2.
- In patients not undergoing surgery: Reduces the pain from hip fractures, provides longer duration of analgesia, reduces the analgesic doses needed and reduces the number of nursing interventions3.
Indications:
Surgical procedures to:
- Hip joint.
- Femur (e.g. femoral fractures)4.
- Knee (e.g. knee arthroscopies, ACL reconstructions, patella ligament realignment)4:
- For anterior knee procedures: A femoral nerve block alone may suffice4
- For coverage of the medial aspect of the knee: Obturator nerve block should be added4
- For coverage of the lateral aspect of the knee: Lateral femoral cutaneous nerve block should be added4
- For coverage of the posterior aspect of the knee: Sciatic nerve block should be added4
- Anterior thigh (e.g. skin graft from the anterior aspect of the thigh) 5.
- Medial aspect of the leg (by blocking the saphenous nerve—a terminal cutaneous branch of the femoral nerve).
- In combination with a popliteal block, analgesia can be provided for any procedure on the lower leg and foot5.
- In combination with a high sciatic block and an obturator nerve block, analgesia can be provided for the entire lower extremity5.
Contraindications:
- Local infection at the proposed needle insertion point.
- Situations where dense sensory block may mask the onset of lower extremity compartment syndrome (especially if combined with a sciatic block). E.g. Fresh fractures of the tibia/ fibula, or extensive and traumatic elective orthopaedic procedures to the tibia and fibula. Best practice will be to consult with one’s surgical colleagues as to the likelihood of compartment syndrome.6
Anatomy:
- The femoral nerve is the largest nerve that arises from the lumbar plexus, which forms within the body of the psoas major muscle.
- It is derived from the anterior rami of nerve roots L2-4.
- It emerges from the lower lateral border of the psoas muscle, descends between the psoas major and iliacus muscles, and then enters the thigh lateral to the femoral artery under the inguinal ligament.
- At the femoral crease, the nerve lies on the surface of the iliacus muscle and is covered by the fascia lata and fascia iliaca. It lies outside of the femoral sheath that contains the femoral vessels.
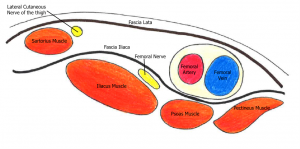
Figure 1: The femoral nerve and its relations in the inguinal region
- Within the femoral triangle, it divides into the anterior and posterior divisions:
- Anterior division
- Sensory: Intermediate & medial cutaneous nerves of the thigh
- Motor: Pectineus & sartorius
- Posterior division
- Sensory: Saphenous nerve
- Motor: Quadriceps femoris
- Articular branches to the hip and knee
|
Dermatomal innervation5: Antero-medial thigh ((femoral nerve), knee (femoral nerve), medial aspect of the leg below the knee down to the foot (saphenous) Myotomal innervation5: Sartorius, Quadriceps Femoris (rectus femoris, vastus lateralis, intermedius and medialis), Pectineus, Iliopsoas Osteotomal innervation5: Anterior wall of hip joint, anterior aspect of femur, anteromedial walls of knee joint |
Sonocharacteristics of the femoral nerve:
- Usually fairly superficial.
- Under the fascia lata (most superficial) and fascia iliaca (immediately adjacent to the nerve & separates the nerve from the artery).
- Lateral to the femoral artery and vein.
- Triangular shaped or oval/ flattened as the nerve fans out into multiple branches.
- Speckled and hyperechoic.
- Becomes less obvious as it branches out caudally.
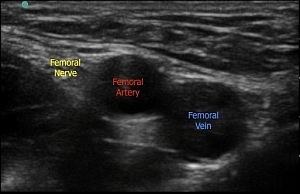
Figure 2: Sonoanatomy of the femoral nerve
Practical conduct of the block:
- Position the patient supine with mild abduction of the ipsilateral leg.
- Attention should be paid to ergonomics to facilitate successful block placement. Position the ultrasound machine so that visualisation of the screen, ultrasound probe and the operator’s hands can be done without needing to turn one’s head. This may be achieved by placing yourself on the side to be blocked and the machine on the far side of the patient.
- Choose a high frequency linear probe (the femoral nerve is fairly superficial).
- Place the probe along the line of the inguinal crease.
- Begin by identifying the circular, anechoic and pulsating femoral artery at the level of the inguinal crease. If this is not immediately visible:
- Slide the transducer medially or laterally
- Check the depth setting
- Use colour flow Doppler to help identify the vessels.
- If 2 arteries are seen, move your probe cephalad.4
- The nerve usually appears as a hyperechoic speckled triangular or oval shaped structure lateral to the artery.
- Follow the nerve along its course to locate where it divides (note this can start above the inguinal ligament in some subjects)—aim to block the nerve proximal to this so as to ensure that both the anterior and posterior divisions are blocked. It is also important to follow the nerve proximally and distally to ensure that it is not a lymph node.4 Inguinal lymph nodes also appear hyperechoic and so can be confused with the nerve in short axis view. A nerve is a continuous structure and can be traced while a lymph node is not and can be seen only in a discrete location.5
- Move your probe up and down and left to right, identifying the surrounding structures and their relationships.
- Prepare the skin and assemble your needle/ syringe/ local anaesthetic. A 22g 50mm needle is usually adequate.
- STOP BEFORE YOU BLOCK.
- An In Plane, lateral to medial approach is preferred.
- Advantages:7
- Able to see the length of the needle and the needle tip during advancement.
- As the nerve is lateral to other structures, it can usually be reached without accidental vascular puncture.
- Disadvantages:7
- Longer course through tissues, so a longer needle may be needed.
- Less convenient for threading a catheter.
- Pierce the needle through the skin on the lateral side of the probe and advance forward towards the femoral nerve. As the needle pierces the fascia iliaca, a “pop” sensation may be felt.
- Aim to place the needle tip immediately adjacent to the lateral aspect of the femoral nerve, into the wedge-shaped tissue space lateral to the femoral artery.
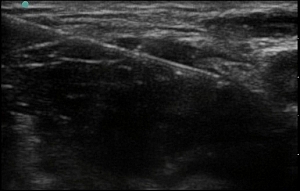
Figure 3. Needle placed into the wedge-shaped tissue space lateral to the femoral artery, lateral to the femoral nerve
- Aspirate before injection. Inject the local anaesthetic in small aliquots with intermittent aspiration, observing the image for local anaesthetic spread and the patient for signs of discomfort (if awake) or toxicity.
- Never inject against a high resistance—this may indicate intraneural needle placement.
- Spread should be visualised below the fascia iliaca and ideally surrounding and highlighting the nerve (“doughnut sign”).
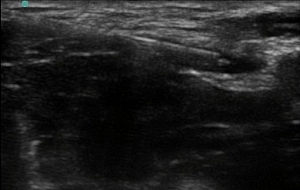
Figure 4: Needle repositioned above the nerve, aiming to surround the femoral nerve with a “doughnut” of local anaesthetic
- Due to contrast enhancement, the hyperechoic nerve often becomes more prominent after injection of hypoechoic local anaesthetic.
Complications:
- Infection
- Vascular puncture and intravascular injection
- Haematoma
- Nerve injury, including intraneural injections
References:
1. Marinković D, Simin J, Drasković B, Kvrgić I, Pandurov M. Efficiency of ultrasound guided lower limb peripheral nerve blocks in perioperative pain management for knee arthroscopy in children. A randomized study. Med Pregl. 2016;69(1-2):5-10.
2. Schloss B, Bhalla T, Klingele K, Phillips D, Prestwich B, Tobias J. A retrospective review of femoral nerve block for postoperative analgesia after knee surgery in the pediatric population. J Pediatr Orthop. 2014;34(4):459-61
3. Turner A, Stevenson M, Cross K. Impact of ultrasound-guided femoral nerve blocks in the pediatric emergency department. Pediatr Emerg Care. 2014;30(4):227-9
4. Flack S, Anderson C. Ultrasound guided lower extremity blocks. Paediatr Anaesth. 2012;22(1):72-80.
5. Szucs S, Morau D, Iohom G. Femoral nerve blockade. Med Ultrason. 2010;12(2):139-44.
6. Murray J, Derbyshire S, Shields M. Lower limb blocks. Anaesthesia. 2010;65(Suppl 1):57-66
-
Jeyaraj S, Pepall T. Ultrasound guided femoral nerve block. Anaesthesia tutorial of the week 284. Available from: https://www.aagbi.org/sites/default/files/284%20Ultrasound%20Guided%20Femoral%20Nerve%20Block.pdf (accessed 10 May 2017)